- Anatomical terminology
- Skeletal system
- Joints
- Muscles
- Heart
- Blood vessels
- Nervous system
- Respiratory system
- Digestive system
- Lymphatic system
- Female reproductive system
- Male reproductive system
- Endocrine glands
- Eye
- Ear
- test
Palate
The palate (Latin: palatum) is a part of the digestive system that is located in the head. It separates the nasal cavity from the oral cavity, as it forms the roof of the oral cavity proper and the floor of the nasal cavity. The palate is composed of two parts - the hard palate (Latin: palatum durum) anteriorly and the soft palate (Latin: palatum molle) posteriorly.
The hard palate forms the bony roof part of the oral cavity, and it is covered by the periosteum and firmly fused with the mucosa. In contrast, the soft palate is the posterior continuation of the hard palate. Opposite it, the soft palate does not have a skeleton made of bones. Instead, the soft palate is the muscular portion of the palate. Both palates participate in digestion, swallowing, breathing, articulation and speech formation.
Hard palate anatomy
The hard palate is immobile and horizontal oriented anterior two-thirds of the palate. It is formed by the bones of the skull connected with the sutures. The bones of the hard palate contain several openings that transmit various nerves and blood vessels. The hard palate borders with the maxillary teeth anterior and lateral, but the soft palate is posterior to it. It has two surfaces - the oral surface facing the oral cavity and the nasal surface directed against the nasal cavity.
Bones and sutures
The bony frame of the hard palate is formed by the horizontal plates of the palatine bones and the palatine processes of the maxillae. The palatine bones are located posterior to the palatine processes of the maxillae, and all structures are covered by the mucosa. The maxillae make up the majority of the hard palate - around two-thirds. In the midline, between both palatine bones and maxillae goes sagittal oriented median palatine suture, while the transverse palatine suture marks the horizontal junction between the maxillae and palatine bones. Overall, the hard palate separates the oral cavity from the nasal cavity.
The hard palate can be subdivided into two parts - the primary palate and the secondary palate. Both portions are separated by the incisive suture resembling the letter "V." The incisive suture begins between the upper lateral incisor and canine teeth on both sides. The left and right suture lines connect at a common site posterior to the incisive foramen. The primary hard palate is the smallest part located anterior to the incisive foramen. In contrast, the secondary palate is the rest of the hard palate situated posterior to the primary palate and anterior to the soft palate.
Landmarks
The anterior aspect of the mucosa forms several ridges going in the transverse directions - palatine rugae. The mucosa of the hard palate also presents the median raphe that corresponds to the median suture. It begins in the middle between maxillary central incisors and extends into the soft palate, dividing the palate into the right and left sides. Bones of the hard palate present with several palatine grooves - impressions from palatine vessels.
Openings
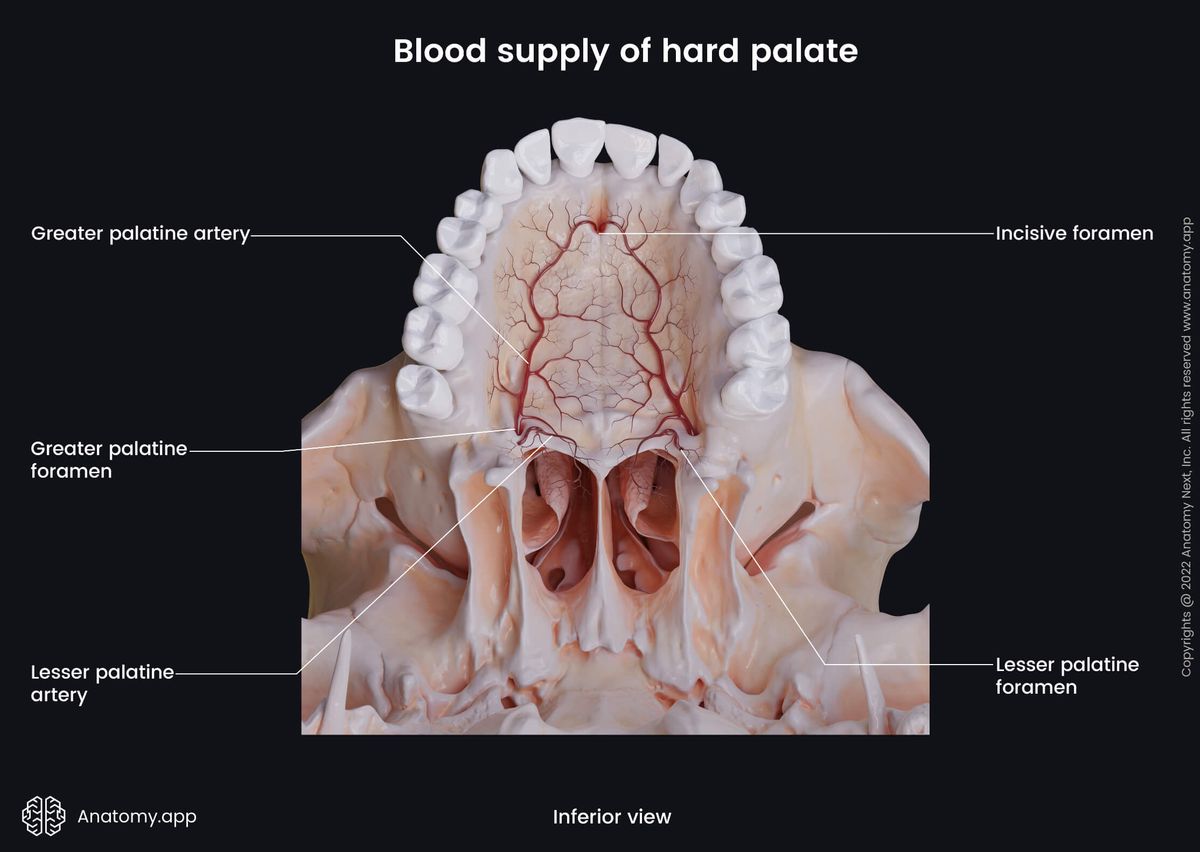
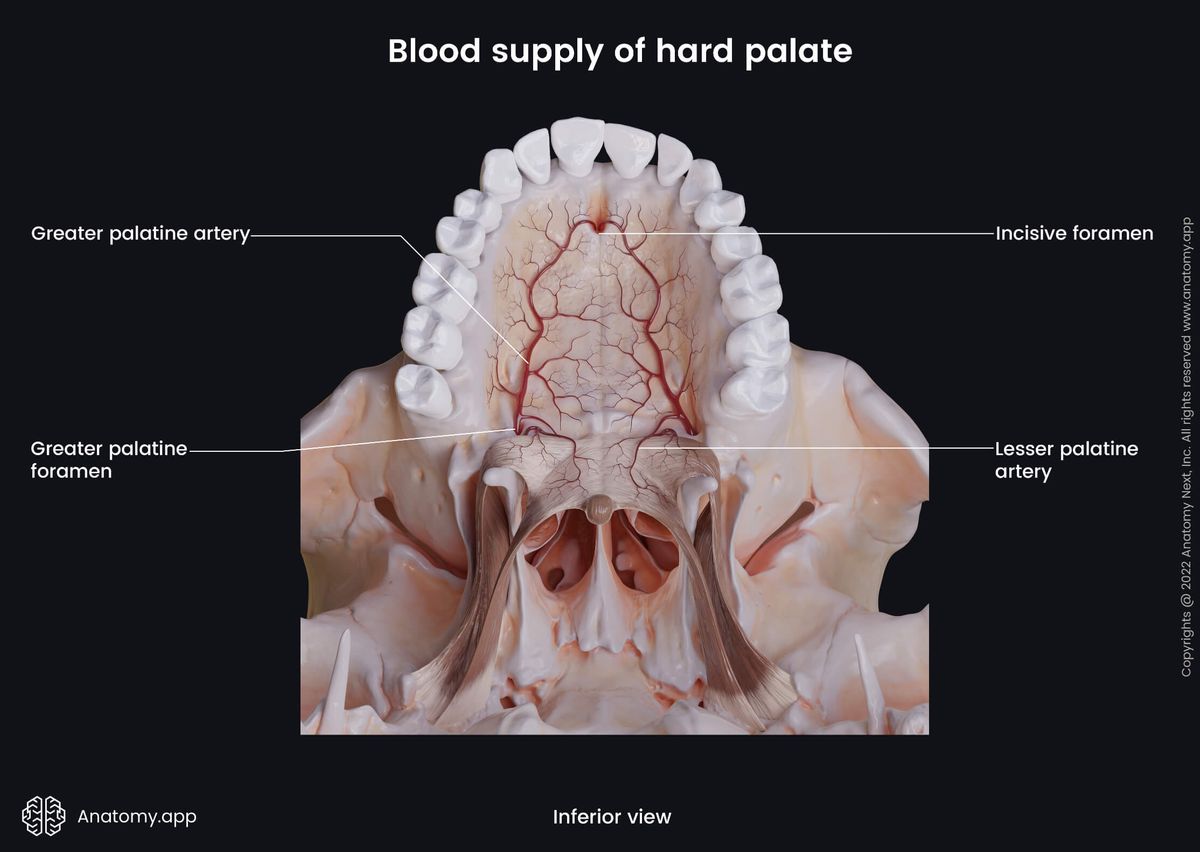
In the midline posterior to both maxillary central incisors is the incisive papilla overlying the incisive fossa or foramen that leads into the incisive canal. The nasopalatine nerve, sphenopalatine artery and terminal branches of the greater palatine artery go through the incisive canal. Besides the incisive foramen, the posterior part of the hard palate has two pairs of foramina - greater and lesser palatine foramina.
The greater palatine foramen is situated in the palatine bone posterior and lateral to the site where the palatine bone and maxilla meet. The greater palatine foramen is located close to the third maxillary molar tooth, and it transmits the greater palatine nerve and blood vessels. The lesser palatine foramen is located behind the greater palatine foramen in the pyramidal process of the palatine bone, and it transmits the lesser palatine nerve.
Soft palate anatomy
The soft palate is a continuation of the hard palate, and it is positioned posterior to it. The soft palate forms around one-third of the palate. It is very mobile, elastic and durable. Like the hard palate, the soft palate also has several landmarks and two surfaces - the oral surface facing the oral cavity and the nasal surface directed against the nasopharynx.
The soft palate borders with the hard palate anteriorly and superiorly. While posteriorly and inferiorly, it has a free margin extending in the oropharynx. On the sides, the soft palate connects with the root of the tongue and lateral walls of the oropharynx. The main components of the soft palate are muscles. Therefore it is also known as the muscular palate.
Landmarks
The anterior aspect of the soft palate is horizontal-directed, while the posterior part is vertical-oriented as it hangs down from the anterior part. The soft palate is also called the velum palatinum. It ends with a free edge that contains an elongated growth in the middle - the uvula. The uvula helps to separate the oropharynx from the nasopharynx.
The lateral sides of the uvula form two arches connecting the tongue and pharynx with the soft palate. The anterior arch is the palatoglossal arch. It is located more anteriorly and ends at the root of the tongue. The posterior arch is the palatopharyngeal arch, located posterior to the previous arch and ending within the lateral sides of the oropharynx.
Both arches sometimes are called faucial pillars or pillars of fauces. The uvula and both arches form the superior and lateral aspects of the oropharyngeal isthmus (isthmus of fauces) - an opening connecting the oral cavity with the oropharynx. Between both arches on either side of the oral cavity is the tonsillar fossa containing lymphoid tissue aggregation known as the palatine tonsil.
Palatine aponeurosis
The soft palate is mainly formed by palatine aponeurosis, skeletal muscles and mucosa. The palatine aponeurosis is a connective tissue plate that begins at the posterior border of the palatine bones and goes in the longitudinal direction across the entire length of the soft palate. It forms the base of the soft palate and connects with its muscles.
Palatine muscles
The soft palate contains five palatine muscle pairs that are essential during swallowing, breathing and articulation. The palatopharyngeus muscle is primarily involved in breathing, while the tensor veli palatini, musculus uvulae, levator veli palatini and palatoglossus - in swallowing.
- The tensor veli palatini originates from the cartilaginous part of the auditory tube and medial pterygoid plate of the sphenoid bone. Fibers of this muscle insert into the palatine aponeurosis. The tensor veli palatini stretches and tenses the soft palate and expands the auditory tube during swallowing.
- The musculus uvulae elevates and shortens the uvula. It arises from the palatine aponeurosis and posterior nasal spine of the palatine bone and ends in the uvula.
- The levator veli palatini elevates the soft palate during swallowing. It originates from the inferior surface of the petrosal part of the temporal bone and the cartilaginous part of the auditory tube. The levator veli palatini muscle inserts into the palatine aponeurosis.
- The palatoglossus originates from the palatine aponeurosis and goes within the palatoglossal arch until it reaches the lateral sides of the root of the tongue, where it inserts. The muscle narrows the oropharyngeal isthmus, shortens the palatoglossal arch and pulls the soft palate towards the tongue.
- The palatopharyngeus shortens the palatopharyngeal arch, narrows the oropharyngeal isthmus and tenses the soft palate. It also moves the pharynx in superior and anterior directions during swallowing. Fibers of the muscle originate from the palatine aponeurosis and hard palate. They go within the palatopharyngeal arch and insert into the lateral sides of the pharynx and the superior border of the thyroid cartilage.
Palate histology
The mucosa of the hard palate usually has a light pink color, while the mucosa of the soft palate appears darker and a bit yellowish pink in color. The palate presents with two different types of mucosal epithelium. The nasal surfaces of the hard and soft palates are covered with the respiratory epithelium. It is a continuation of the nasal mucosa lined with the ciliated epithelium. The oral surface of the soft palate is a continuation of the oral mucosa of the hard palate. The histology of both palates is slightly different.
Hard palate
During mastication, the oral surface of the hard palate is subject to mechanical forces by various factors. Therefore it is lined with the stratified squamous keratinized or partially keratinized epithelium. The epithelium is closely fused with the connective tissue. Deep within the connective tissue in the anterior aspect of the hard palate are located many fat cells. The middle and posterior portions contain a considerable amount (around 250) of mixed and mucous minor salivary glands. Around the median raphe, the connective tissue layer is thin, and it has a close and strong connection with the periosteum. The nasal surface is lined with the ciliated pseudostratified columnar epithelium containing mucus-producing goblet cells.
Soft palate
The soft palate contains a significant amount of collagen and elastin fibers. Its oral surface is lined with the stratified squamous non-keratinized epithelium. Usually, the soft palate of a child contains taste buds, while adults rarely have them. Connective tissues are very vascular. The soft palate contains mixed and mucous minor salivary glands with a more significant amount in the uvular part. The nasal surface is lined with the ciliated pseudostratified columnar epithelium, containing mucus-producing goblet cells. The uvular part is covered by the stratified squamous non-keratinized epithelium.
Palate functions
The palate is involved in several physiological processes, and it mainly assists during digestion, articulation, breathing and speech formation. The hard palate is primarily involved in digestion and speech formation, while the soft palate takes part in swallowing and breathing.
Hard palate
The hard palate provides functions associated with the digestion, articulation and speech formation, and they include the following:
- The structure of the hard palate allows it to participate in the mastication process as it withstands mechanical forces during chewing. Also, the hard palate helps to form the food bolus (chewed food that is mixed with the saliva). The palatine rugae provide more efficient chewing and food bolus formation.
- It holds the food while it is within the oral cavity.
- The hard palate provides slight changes in the pressure within the oral cavity when the nasal passages are closed. Therefore, for newborn babies, it ensures suckling and breastfeeding.
- The interaction of the tongue and hard palate is associated with certain speech sounds, such as the letter "T" or "D."
- And finally, the hard palate separates the nasal cavity from the oral cavity.
Soft palate
The soft palate is responsible for functions related to digestion and breathing, and they are as follows:
- The soft palate is moveable and contains many muscles. It is responsible for the closing and opening of the oropharyngeal isthmus. Therefore the soft palate separates the oropharynx from the nasopharynx during swallowing. It prevents food and fluid regurgitation from the oropharynx into the nasopharynx and airways.
- It also acts very similarly when a person sneezes as it closes the nasal passage, and the flow of the secretion is directed only towards the oral cavity.
- The soft palate provides the oral speech sounds without nasal sounds by separating the nasal cavity from the oral cavity.
- The interactions of the soft palate and tongue form several speech sounds, such as the letters "N" and "K."
- The palate is mainly innervated by the branches of the vagus nerve (CN X), and the uvula is involved in the gag reflex. Touching the uvular part can cause the reflex and subsequent vomiting. Therefore, the palate also has a protective function.
- The soft palate provides breathing when the mouth is closed.
- The soft palate is responsible for snoring. Snoring is a partial obstruction of the airways caused by gravity, relaxation of the muscles and movements of the soft palate during breathing while sleeping.
Neurovascular supply of palate
Arterial blood supply
The arterial blood supply of the palate is mainly provided by two arteries - the ascending and descending palatine arteries. The first one perfuses only the soft palate, while the second artery supplies both palates and muscles of the soft palate. The ascending palatine artery is a branch of the facial artery, and the descending palatine artery arises from the maxillary artery. The descending palatine artery has two branches - the greater and lesser palatine arteries. Multiple arteries supply the palatine tonsil, and they include:
- Tonsillar artery of the facial artery
- Ascending palatine artery of the facial artery
- Dorsal lingual artery of the lingual artery
- Ascending pharyngeal artery of the external carotid artery
- Greater palatine artery of the descending palatine artery
Venous and lymphatic drainage
Venous drainage is provided by the facial vein that drains into the common facial vein, and then venous blood is carried next to the internal jugular vein. Most of the veins of the palate are drained to the pterygoid and tonsillar venous plexuses. Lymph from the soft and hard palate is mainly carried to the deep cervical nodes.
Innervation
The motor innervation of almost all palatine muscles, except the tensor veli palatini, is provided by the pharyngeal branch of the vagus nerve (CN X) via the pharyngeal plexus. The tensor veli palatini muscle is supplied by the medial pterygoid nerve - mandibular division (CN V3) of the trigeminal nerve (CN V).
The sensory innervation is primarily provided by the maxillary division (CN V2) of the trigeminal nerve (CN V) via the greater and lesser palatine nerves and nasopalatine nerve. The greater palatine nerve mostly innervates the hard palate, while the lesser palatine nerve supplies the soft palate.
The palatine tonsil, palatoglossal and palatopharyngeal arches are innervated by the tonsillar nerves coming from the glossopharyngeal nerve (CN IX). The greater petrosal nerve from the facial nerve (CN VII) and the lesser palatine nerve carry information about taste sensations from the taste buds found in children.
Cleft palate
Cleft palate is among the most common orofacial congenital disabilities, mostly affecting the hard palate, but it can also involve the soft palate. It is formed during the embryological development around weeks sixth to ninth. During development, the palatine processes of the maxillae and horizontal plates of the palatine bones do not fuse properly together, leaving a gap between them. It can happen partially or entirely. This condition often presents together with the cleft lip - a gap in the lip.
The cleft palate can be an isolated disorder, but it can also be associated with other genetic diseases like Edwards syndrome (18 chromosome trisomy). Isolated cleft palate most often affects girls, but cleft lip - boys. Babies with cleft palate have visible facial deformities, and they have problems with proper breathing, feeding and speech that can result in malnutrition and growth retardation. If the condition is left untreated, there can be difficulties with speech formation later. Children with cleft palate often have recurrent middle ear infections, hearing problems and teeth issues.
Risk factors
The risk factors for cleft palate are often unidentified, but some linked relations are probably causing the condition. Cleft palate is a multifactorial disorder, meaning it is caused by the changes in genes and environmental factors of the mother, such as medication usage and eating and drinking habits. The chance for a baby to have cleft palate increases with the following factors:
- Positive family history of cleft palate or lip
- Smoking during the pregnancy
- Drinking alcoholic beverages during the pregnancy
- Medication usage during pregnancy (most often, this condition is caused by medications used to treat epilepsy or folic acid antagonists (methotrexate))
- Diabetes
- Obesity during pregnancy
Variations
The cleft palate can present as a unilateral condition, affecting just one side of the palate, or it can develop on both sides and then it is known as bilateral cleft palate. Three types of cleft palate can be present: complete, incomplete and submucosal cleft palate.
In the first variation, the disorder affects the hard and soft palate and also the uvula. The incomplete variation presents with clefting in the secondary palate of the hard palate. The mucosa is intact in the submucosal cleft palate, but the underlying muscle part is defective.
Diagnosis and treatment
Cleft palate can be diagnosed before the child is born by imaging studies such as the ultrasound, or it can be detected after the baby is born by physical examination. Treatment depends on the variation and severity of the condition and other presenting disorders.
Cleft palate usually is treated between six to twelve months, and healthcare professionals recommend repairing the defect within the first 18 months. After successful surgery, most children born with cleft palate will not have any issues later in their lives.
Anatomy.app
Contact information
- For questions regarding business inquiries. Please contact:
- info@anatomy.app